





Thanks to their unique laser sintering process, the translucent enamel and occlusion veneers (edelweiss VENEER & OCCLUSIONVD) stand out due to their inorganic, ceramic-like surface vitrification and tempered composite body. The occlusions represent the anatomic foundations for single or complete reconstructions and for increasing the vertical dimension (OVD) in the posterior region. Hence, a functioning anterior cusped guidance can also be obtained using edelweiss „VENEERs“.

edelweiss dentistry
edelweiss OCCLUSIONVD
Sale price
Price
€67,20
Regular price
Unit price
per
Tax included.
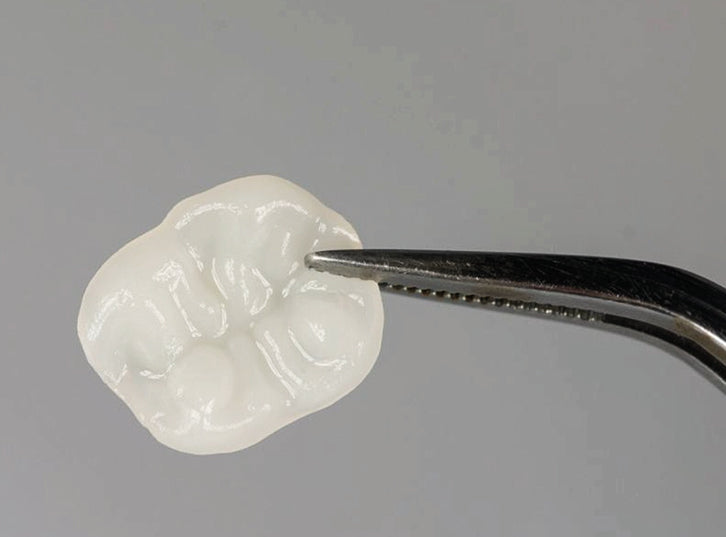
Onlays/occlusions are polymerized, laser-machined, prefabricated, radiopaque, highly filled nano-hybrid composite enamel occlusal shells. The occlusal and anatomical shape template in the form of a thin enamel shell facilitates direct veneering of single or multiple posterior teeth.
Reconstruction is quick and easy with an esthetic, functional and high-quality result. Onlays/occlusions are cemented in place with the same material they are made of, creating a stable unit, the entire restoration (between dentin/enamel + composite + onlays/occlusion) Onlays/occlusions allow simple and complex posterior restorations with a biomechanical result.
The prefabricated onlays/occlusions provide the anatomical basis for single or complete reconstructions as well as for raising the vertical dimension in the posterior region. Thus, it is also possible to achieve a functioning anterior canine alignment by means of edelweiss VENEERs.
Note: This product is available and approved exclusively for dental customer groups.
Downloads
- Instruction for use
- Fact Sheet
- Brochure
- Step by Step
- Booklet_Step_by_Step
- Indication Guide
- Safety Data Sheet
Composition
- Barium dental glass
- Bis-GMA-based matrix of dental resins
- Pigments
- Additives
- Catalyst
Technical Data
Filler content: 82 wt.% The variation range of the inorganic filler particles is between 0.02-3µm.
Properties edelweiss COMPOSITE
(which is recommended for luting and direct filling therapy)
- User-friendly handling
- Excellent processing properties
- Easy and fast polishability
- Low shrinkage due to the use of nano technology and a high filler content(83%)
- Excellent abrasion behavior
- Very good physical properties
- Antibacterial surface due to zinc and furfural content in the filler
- Natural fluorescence
Indications
- Anterior and posterior restorations
- Tooth discolorations
- Anatomical deformities
- Diastema
- Erosion & Attrition
- Customized Veneers, Crowns & Bridges
- Crowns & Crown facings
- Increasing the vertical dimension (CMD)

The best for your patients
«By combining and adapting of the latest composite and laser technology, edelweiss dentistry has made a quantum leap into the future of minimally invasive dentistry. The laser process combines the best of two worlds: an homogeneous, inorganic and maximum gloss surface with a thermally tempered and dynamic composite core. Thus, an optimal integration in function and esthetics is achieved. This, combined with maximum cost-effectiveness, has convinced me and my patients.»
“The difference lies in the high similarity with nature.”
The Vertical Dimension

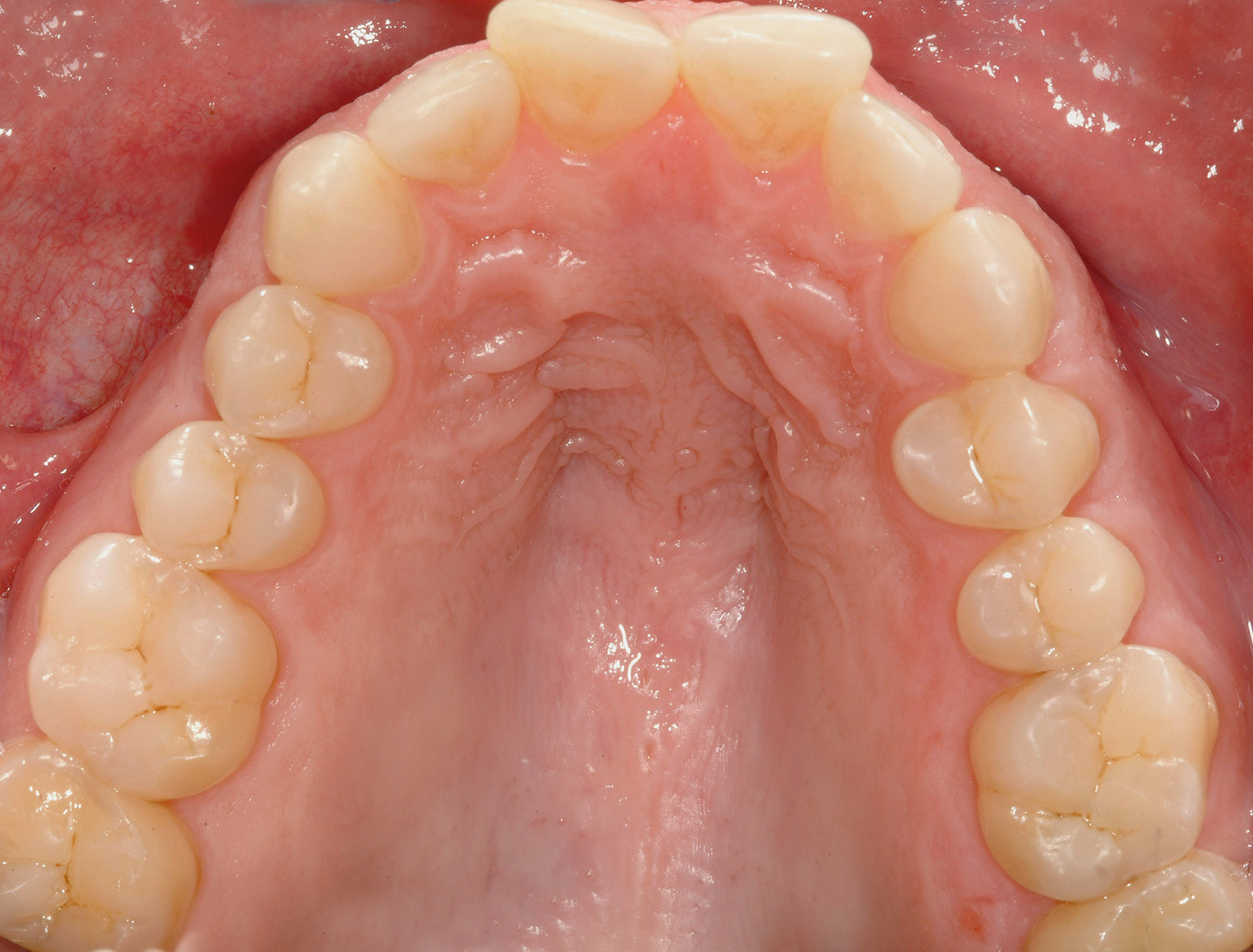
OCCLUSIONVD ENAMEL SHELLS Upper jaw
Adjusted stone model

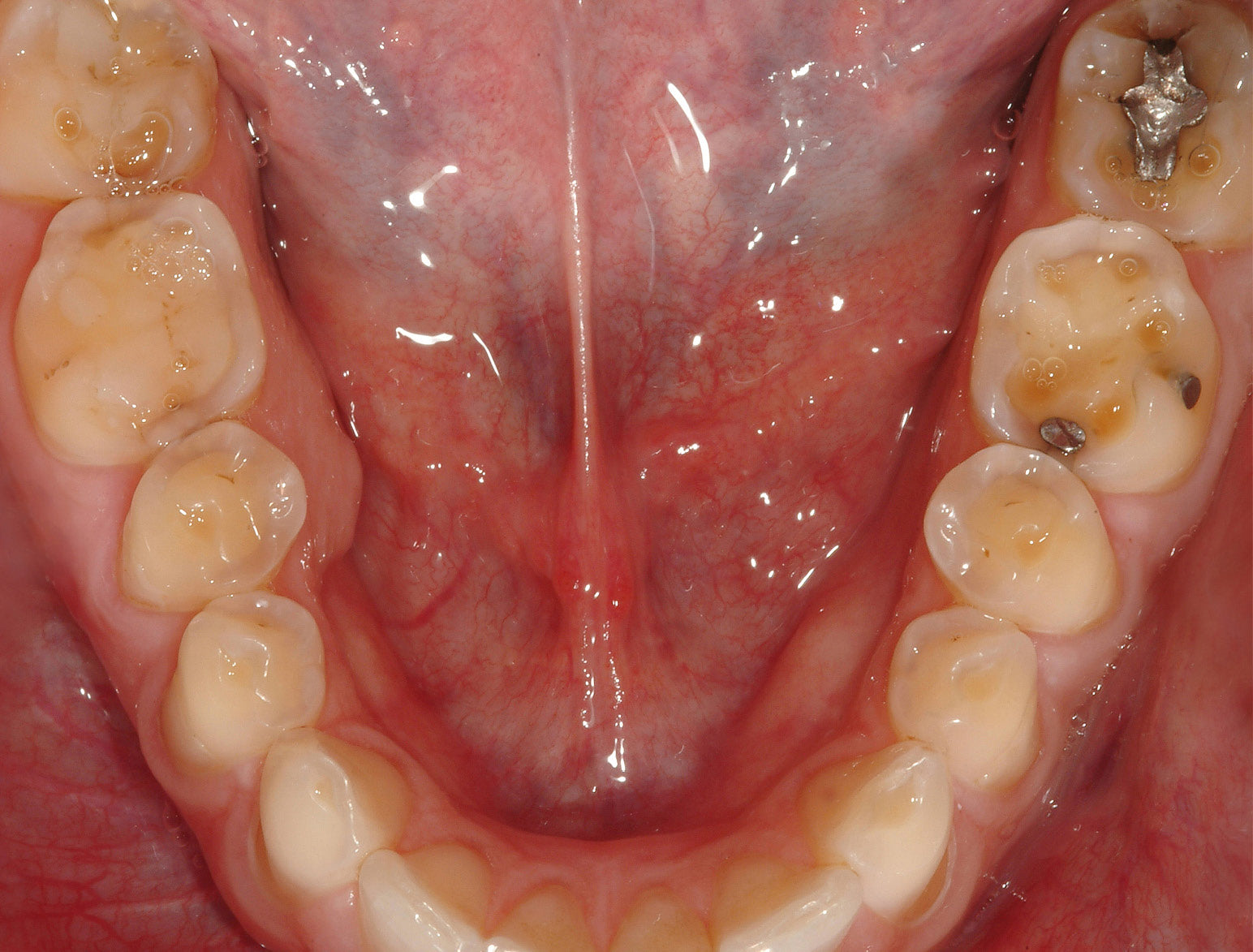
OCCLUSIONVD ENAMEL SHELLS Lower jaw
Adjusted stone model
Function
edelweiss VENEERs & OCCLUSIONVD allow for minimally invasive biomechanical and economical treatment of the cause as well as prevention of cranio-mandibular dysfunction (CMD). Furthermore, malocclusion and deep bites can also be corrected minimally invasively. By covering the occlusal surfaces, usually in the mandible, the mandible is brought into the correct position for the patient in relation to the maxilla. This makes it possible to attain functioning guidance of anterior teeth and cuspids by using edelweiss VENEERs.
Lifting the Vertical Dimension
Using edelweiss occlusal surfaces. In most cases the mandible is appropriate. It can often be identified by the great difference in height from the cuspid to the premolar (33 to 34 and 43 to 44). However, to ensure that lifting, and protrusion if necessary, is equal on the left and right, this needs to be tested using situation models on the articulator. In the premolar region this can mean capping up to 5 mm, and up to a further 3 mm in the molar region.



Procedure
The maxilla and the mandible models are articulated head-adequate in habitual intercuspation. Protrusion is then performed as required and the supporting pin of the articulator raised. Michigan or Partial bite splints with “stops” are prepared for the mandibular quadrants. These are fixed temporarily in the mouth, in other words, provisionally. After a few weeks this will already represent the ideal position of the mandible, possibly requiring re-occlusion. On the basis of these bite splints the mandible is articulated anew against the maxilla.
Indirect Application
By relining the prefabricated occlusal surfaces on existing model occlusal surfaces with composite, one can simply create a new functioning biomechanical, balanced and smoothly working masticular apparatus without irritations. Then the occlusions are transferred from the model to the patient’s occlusions and attached via bonding and composite.



OCCLUSIONVD ENAMEL SHELLS Lower jaw
Relined and adapted by the dental technician on stone model

Finished OCCLUSIONVD in final situation
Direct Procedure
For advanced professionals: Instead of lining the occlusions on the model in the articulator, a bite registration material (silicone) is used to make an occlusal impression which accurately portrays the clearance between the maxilla and the mandible in the articulator. Using the fixed silicone bite register, direct application of the prefabricated occlusion can be performed. The silicone bite register is in each case placed unilaterally (left or right) on the patient’s occlusion. In other words, when the left quadrant is restored with occlusions, the right quadrant sets the height and position of the bite elevation and thus the final position of the composite-lined and bonded occlusions on the left when biting down (replacing the supporting pin when closing the articulator).
Once the left quadrant has been restored, the right quadrant is treated. Now one can optionally prepare a further silicone register from the quadrant already restored with occlusions (left) in combination with the silicone register (right) already prepared with the articulator, which additionally guides and sets the already attained occlusional relationship between the maxilla and the mandible (left) during biting. Practised users can dispense with this silicone register (for example, on the left) as the patient now already bites on the newly gained occlusion or bite elevation during biting. After setting all occlusions, re-occlusion is performed until the desired contact points have been attained.
Sizes
One size for all
Based on a study of all shape and size variations of natural tooth anatomy, prefabricated and contourable universal occlusion shapes for the upper and lower arches were developed.


Size selection
The selection of the tooth shape is made using the available sizing guide. (OCCLUSIONVD - Sizing Guide). The sizing guide is positioned over the teeth to be restored, and the outline allows for proper selection of the best-fitting occlusion.
Morphology
Ultra-thin, anatomical occlusions in three sizes (S, M & L). The glass component in the composite filler and laser treatment of the surface give the material nature-like mechanical properties (biomechanics), and the material is also biocompatible (biology). Due to the natural morphology, the prefabricated edelweiss Occlusions are very easy to incorporate into an existing occlusion.

Sizing Guides
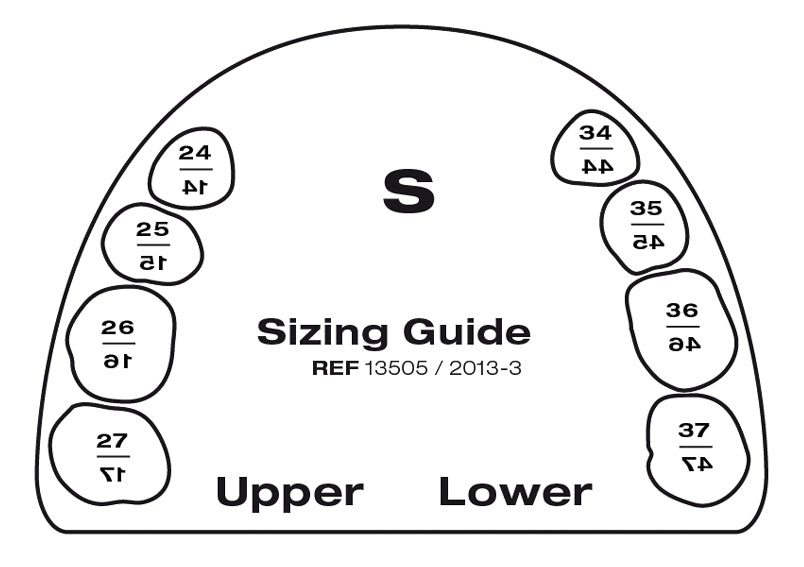
Small
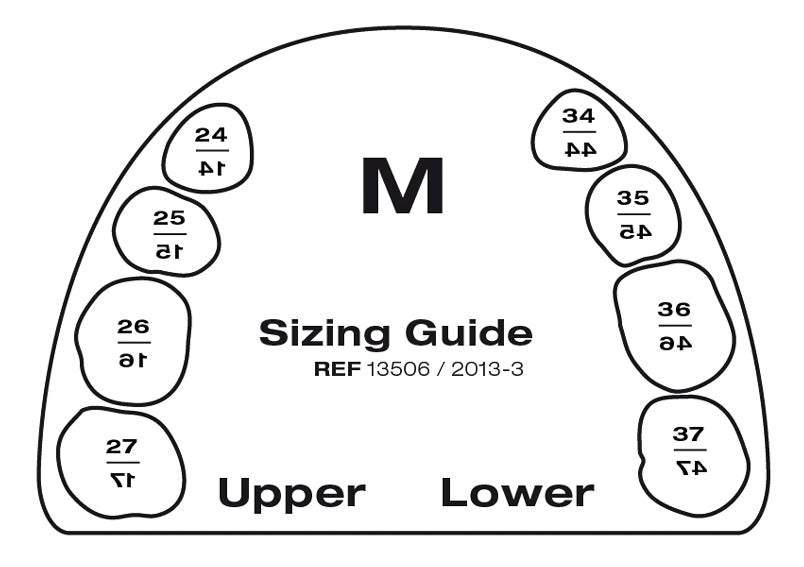
Medium
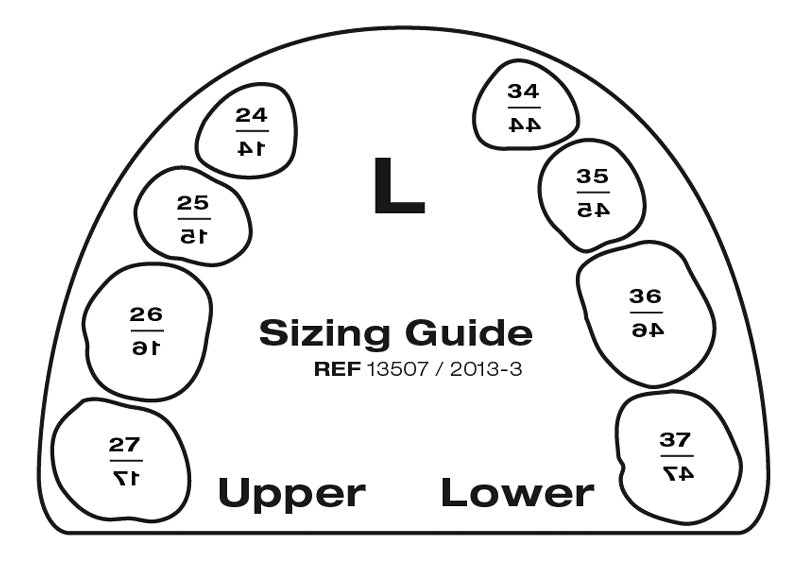
Large
Shade Range

edelweiss Shade Guide
edelweiss dentin and enamel shades based on the natural layering technique.

Shade Selection
Placing the enamel VENEER shell over the dentin core.
For light refraction place glycerine within enamel shell first.
edelweiss Shade System

edelweiss VENEERs & OCCLUSIONVDs consist of the shade Enamel – Vita Enamel AO.
The respective dentin and enamel shades used to cement the VENEER will determine the final shade tone of the restoration.
Example: edelweiss VENEER (Vita Enamel Shade AO) cemented with Dentin Shade A3 (Vita Dentin Shade A3) will result in the Vita Dentin Shade A3.
Standard Restoration - Step by Step
1
Relined and customized OCCLUSIONVD by dental technician.

2
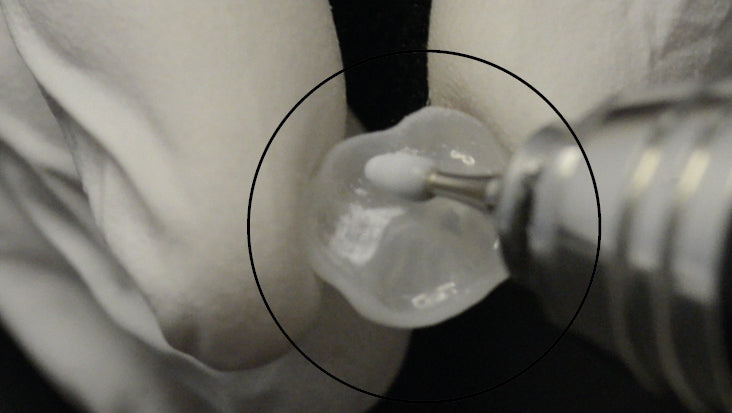
Application of VENEER Bond onto OCCLUSIONVD.

3
Gently air dry inner surface.

4
Light cure for 20 sec. with VALO (UPI) at standard power. With other Light cure for 40 sec.

5
Etching for 30 sec.

6
Bonding (UPI, peak universal) / Floss interproximal areas before light curing with VALO (UPI).
7
Light cure for 20 sec. with VALO (UPI) at standard power. With other Light cure for 40 sec.

8
Application of N.-H. Dentin or Enamel Composite.

9
Adaptation of N.-H. Dentin/Enamel Composite.

10
Positioning and removal of surplus material.
11
Floss interproximal areas then light cure for 20 sec. with VALO (UPI) at standard power. With other Light cure for 40 sec.

12
Finishing of interproximal area.

13
Insertion of the OCCLUSIONVD.

14
Positioning of OCCLUSIONVD and removal of surplus material. Adapt margins.

15
Floss interproximal areas then light cure for 20 sec. with VALO (UPI) at standard power. With other Light cure for 40 sec.

16
Finish and polish margins using fine finishing diamonds and Jiffy polishers.

17
Relaxed bite position in vertical dimension.

18
Front view / space for lower VENEERs.
Individualized Restoration - Step by Step

1
Preoperative situation. Occlusal view.

2
Prepared and roughened crown.
3
Roughen inner surface of the OCCLUSIONVD.
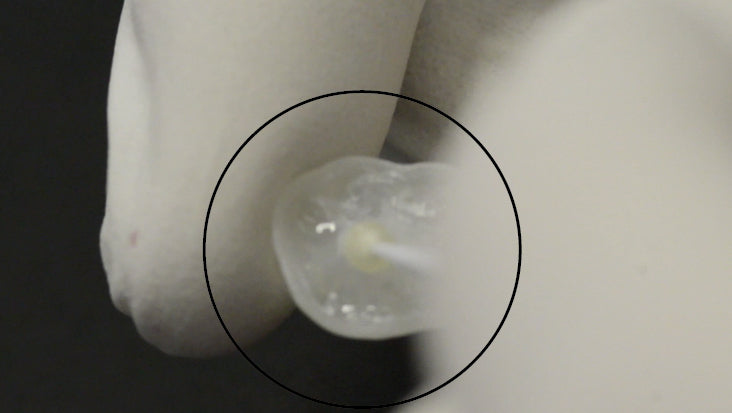
4
Application of VENEER Bond onto OCCLUSIONVD.

5
Light cure for 10 sec. with VALO (UPI) at standard power. With other Light cure for 20 sec.
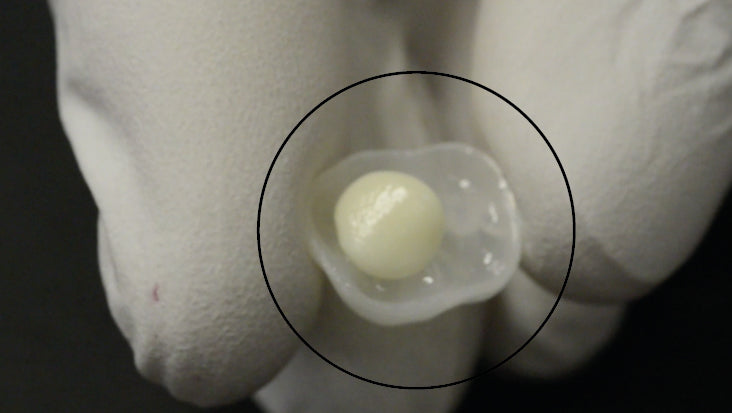
6
OCCLUSIONVD ready for semi direct placement (filled with dentin).

7
Insertion of the OCCLUSIONVD.

8
Positioning and fit check of the OCCLUSIONVD in final occlusal position.

9
Positioning and fit check of the OCCLUSIONVD in final occlusal position.
10
Visual observation.
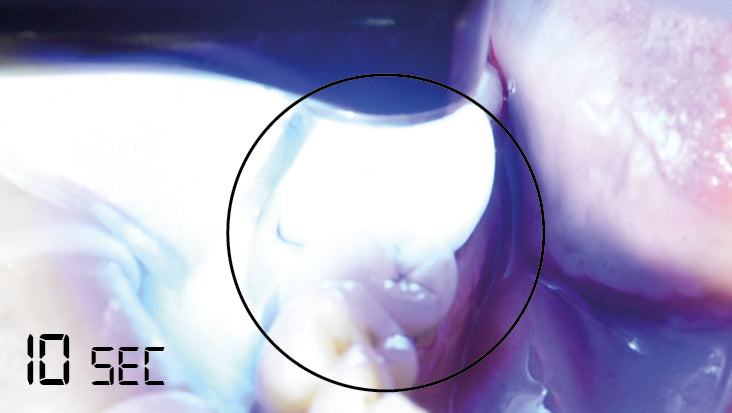
11
Light cure for 10 sec. with VALO (UPI) at standard power. With other Light cure for 20 sec.

12
Visual observation.

13
Removal of the semi direct fitted OCCLUSIONVD.

14
Basic view of the semi direct fitted OCCLUSIONVD.
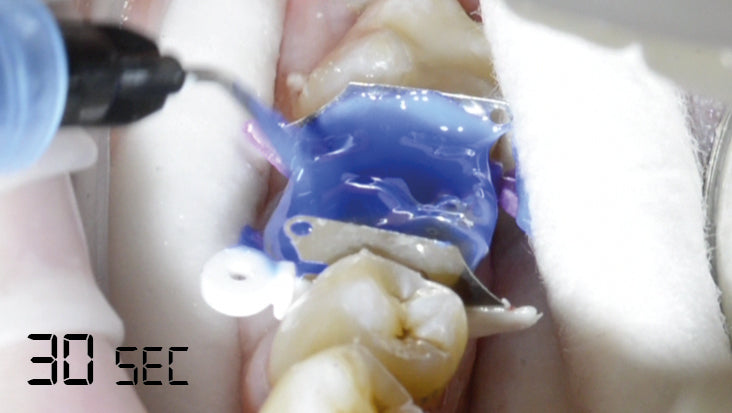
15
Isolation with Wedge Guards and etching for 30 sec.

16
Placing a puddle coat of Bond on crown.
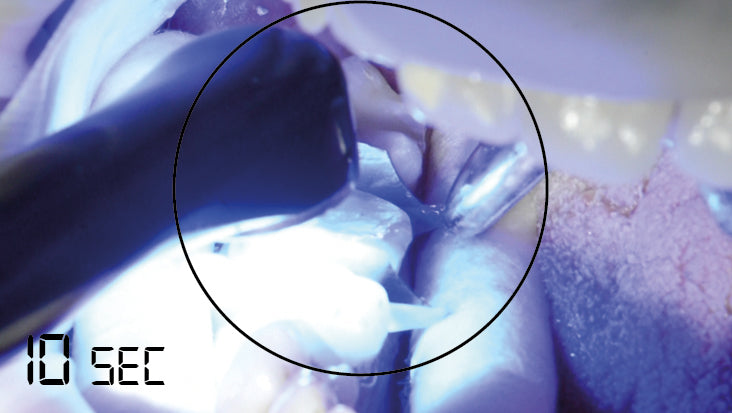
17
Light cure for 10 sec. with VALO (UPI) at standard power. With other Light cure for 20 sec.
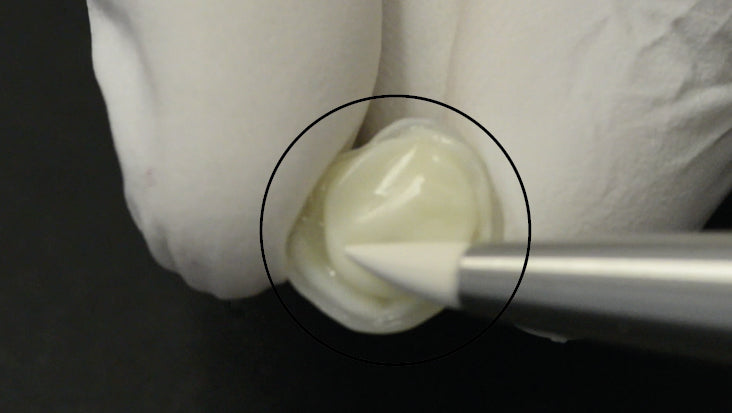
18
Application of N.-H. Dentin or Enamel Composite.
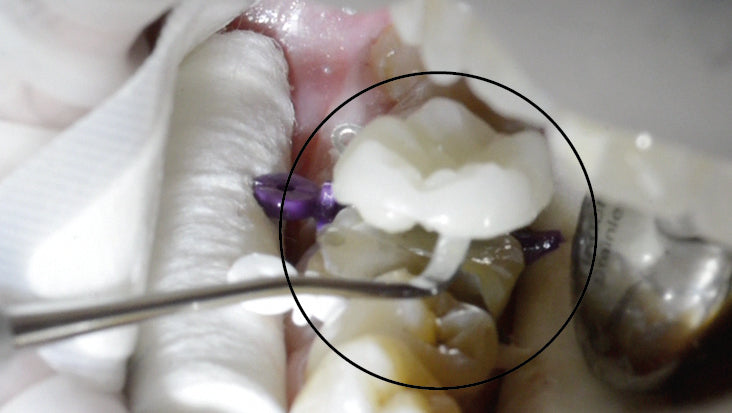
19
Insertion and final positioning of OCCLUSIONVD.

20
Final fit check.

21
Adapt margins. Removal of surplus material.
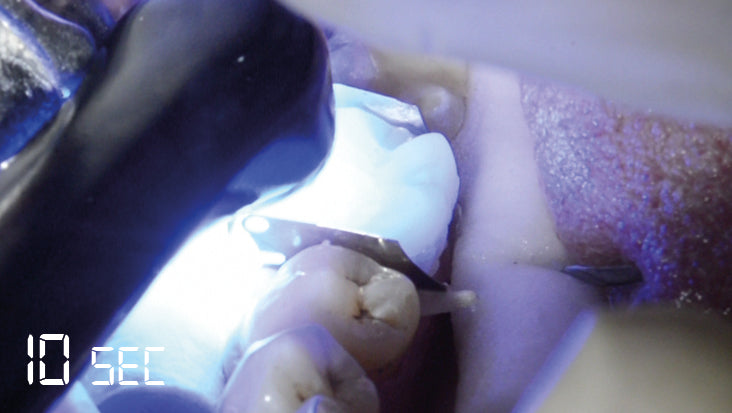
22
Light cure for 10 sec. with VALO (UPI) at standard power. With other Light cure for 20 sec.

23
Removal of Wedge Guards.

24
Finish and polish margins using fine finishing diamonds and Jiffy polishers.
25
Finishing interproximal areas using polishing strip.

26
Visual observation.

27
Reocclusion.

28
Reocclusion.

29
For high shine polish OCCLUSIONVD margins with Jiffy polishers.

30
Final postoperative situation.
Metal Ceramic Crown Repair - Step by Step

1
Preoperative situation.

2
Prepared and roughened crown.

3
Trial fit of OCCLUSIONVD on prepared crown.

4
Trial fit of OCCLUSIONVD on prepared crown.

5
Isolation with ultradent Opal Dam and etching with ultradent ceramic etch.

6
Placing a puddle coat of Peak Univ. Bond (UPI) on crown & inserting dental floss for separation.

7
Light Cure for 20 sec with VALO (UPI) at standard power. With other Light cure for 40 sec.

8
Cover metal area with edelweiss Opaque White Effect Shade.

9
Dispense edelweiss N.-H. Composite onto inner surface of the OCCLUSIONVD.

10
Adapt edelweiss N.-H. Composite into OCCLUSIONVD.

11
Position and press OCCLUSIONVD in place.

12
Adapt edelweiss N.-H. Composite & remove excess.

13
Floss interdental area.
14
Light cure for 20 sec. with VALO (UPI) at standard power. With other Light cure for 40 sec.

15
Visual observation.

16
Reocclusion.

17
Visual observation after reocclusion.

18
Finish cervical and interproximal margins using Soflex Discs.

19
Proof of functional movements.

20
Side view.

21
Occlusal view.
Mechanical Properties
• Good abrasion resistance
• Very good physical and mechanical properties
• Antibacterial surface due to zinc and fluorine particles in the filler
• Easy polishing
• Natural fluorescence and opalescence
|
--> OCCLUSIONVD |
N.-H. Composite |
N.-H. Flowable Composite |
|
|---|---|---|---|
| Flexural Strength | 200 MPa | 150 MPa | 120 MPa |
| Compressive Strength | 550 MPa | 480 MPa | 350 MPa |
| Flexural Modulus | 20 GPa | 12.5 (dentin) - 16 GPa (enamel) | 6 Gpa |
| Surface Hardness | 100 HV | 80 HV | 68 HV |
| Polymerization Shrinkage | - | 2.50 % | N.A. |
(Source: internal data from edelweiss dentistry)
Technical Aspects
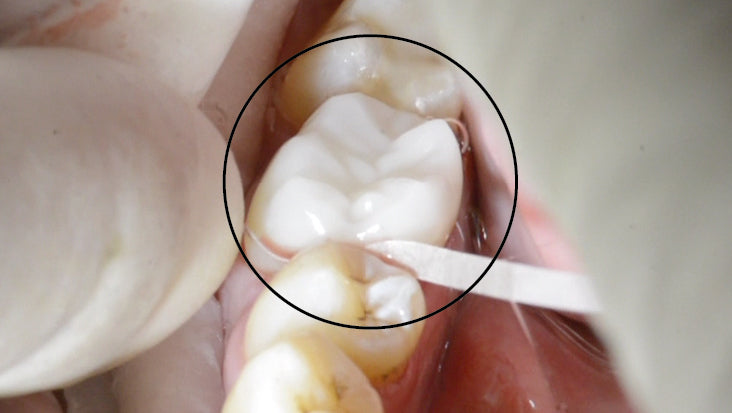
View of a sectioned extracted human molar with a cemented prefabricated composite VENEER / OCCLUSIONVD bonded to half of the enamel surface and the other half to the dentin surface.


The most relevant observation made was obtained upon the evaluation of the inner adaptation of the restoration. No defects were visible at the interface of the enamel or in between the restorative composite and the VENEER / OCCLUSIONVD, which confirmed the excellent bond strength and stability at both interfaces (dentin/enamel to composite, composite to VENEER / OCCLUSIONVD).
Fatigue Behavior
Fatigue behavior for composite VENEER / OCCLUSIONVD: A recent in vitro study demonstrated that prefabricated composite VENEER / OCCLUSIONVD cemented onto the enamel and dentin surface of molars, effectively resisted simulated functional fatigue and load testing. Virtually no defects were observed at both the enamel and dentin margins, either before or after loading, which typically represents the most vulnerable area of a restoration.
UNIVERSITÉ DE GENÈVE
Prof. Dr. Didier Dietschi D.M.D, PhD, Privat-Docent Specialist SVPR Assoc. Professor
Repairability






Clinical Cases - Step by Step

Case 1 A / left
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 A / right
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 B / left
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 B / right
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 C / Upper jaw
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 C / Lower jaw
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 D / Before
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 D / After
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 E / Before
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 E / After
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 F / Before
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 F / After
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 G / left
Congenital Amelogenesis Imperfecta Hypomatuation

Case 1 G / right
Congenital Amelogenesis Imperfecta Hypomatuation

Case 2 A / Before
Posterior restorations
Case 2 A / After
Posterior restorations
Case 2 B / Before
Posterior restorations

Case 2 B / After
Posterior restorations

Case 3 A / Before
Full mouth rehabilitation

Case 3 A / After
Full mouth rehabilitation

Case 3 B / Before
Full mouth rehabilitation

Case 3 B / After
Full mouth rehabilitation

Case 3 C / Before
Full mouth rehabilitation

Case 3 C / After
Full mouth rehabilitation

Case 3 D / Before
Full mouth rehabilitation

Case 3 D / After
Full mouth rehabilitation

Case 3 E / Before
Full mouth rehabilitation

Case 3 E / After
Full mouth rehabilitation

Case 3 F / Before
Full mouth rehabilitation

Case 3 F / After
Full mouth rehabilitation

Case 3 G / Before
Full mouth rehabilitation

Case 3 G / After
Full mouth rehabilitation

Case 4 A / Before
Lifting the vertical dimension

Case 4 A / After
Lifting the vertical dimension

Case 4 B / Before
Lifting the vertical dimension

Case 4 B / After
Lifting the vertical dimension

Case 4 C / Before
Lifting the vertical dimension

Case 4 C / After
Lifting the vertical dimension

Case 4 D / Before
Lifting the vertical dimension

Case 4 D / After
Lifting the vertical dimension

Case 4 E / Before
Lifting the vertical dimension

Case 4 E / After
Lifting the vertical dimension